Having 2 of the 4-member team nipping off to the neonatal unit in the middle of the day is not easy on the 2 left behind holding the baby – literally. Jarlath and Kirstie have been doing sterling work covering for our disappearing acts.
Kirstie trying to time keep for Jarlath. “I’ve never been one to miss an educational opportunity” – even if it means adding 5 minutes to the lectureJarlath’s lecturing aids – you hold this side up if you have a question and you show the red dot if the lecturer is speaking too fast or you don’t understand
At one point, we came back to the lecture theatre to find that Jarlath’s lecture on convulsions had attracted a 16th learner.
Black-cheeked, white-nosed monkeyAlso known as the red-tailed guenon
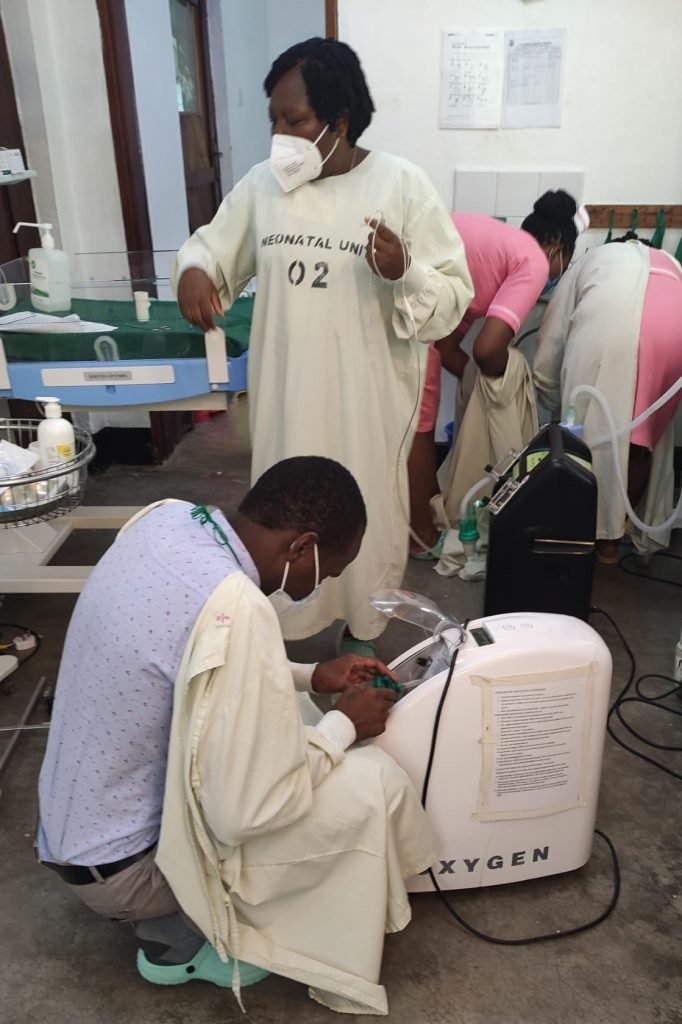
Grace directing Ugandan health professionals in how to make homemade CPAP
A premature baby (probably about 28 weeks gestation) was born on our first day in Bwindi. He weighed 1kg (2.2lbs). The paediatrician had just left the hospital and we were asked to help the young doctor pictured above who was covering the paediatric unit. Grace and Julia have visited daily for the last 5 days and supported the nurses in their excellent care of the tiny little boy who is now off CPAP and in skin to skin care with his mother for much of the day. It is normal for these babies to lose up to 10% of their birthweight and he now weighs 890g but is tolerating his expressed breast milk and I would expect him to start to put on weight from now on. He has had no blood tests, no x-rays and only homemade CPAP to support his breathing. He is a shining example of what good nursing care can do and we have used him throughout the course to illustrate what we teach about supporting preterm babies. These are the lives that can be saved by teaching staff the Neonatal Care Course.
Julia attending to the 28 week gestation baby on the neonatal unit
Some of the successful learners from the second NCC with their certificates
We have been made most welcome here in Uganda for the first 2 Neonatal Care Courses and have been very impressed with the standard of care at Bwindi Community Hospital and the thirst for knowledge amongst the health professionals here.
We have identified 12 potential instructors and aim to return in November to run a Generic Instructor Course and 2 more Neonatal Care Courses. Fund raising over the next few months will be aimed at this next step of the 10 steps to sustainability plan.
My favourite lecture is the one on jaundice – a pet topic of mine. I was challenged today on my statement that congenital malaria can cause jaundice. Actually the challenge was whether the malaria parasites can cross the placenta. Grace – with a lot more experience of congenital malaria than me – came to my rescue. In Cameroon, she is now doing peripheral blood smears for babies born to mothers known to have malaria during delivery and is finding more cases than expected in the neonates being treated for sepsis. This evening, I looked it up.
Here are a few bullet points from the above paper which comes from just east of where I am sitting as I write:
placental malaria significantly increases the risk of perinatal morbidity and mortality including low birth weight, intrauterine growth restriction, preterm labour and intrauterine fetal death
malaria in pregnancy is estimated to account for 100,000 neonatal deaths annually
maternal malaria can be prevented during pregnancy with intermittent presumptive treatment with sulfadoxine–pyrimethamine, and can reduce neonatal mortality by up to 61%
maternal immunity to malaria may confer protection to the fetus through transmission of immunoglobulin G antibodies (IgG) against malaria
the presence of fetal haemoglobin (HbF) in the neonate prevents high parasitaemia
to maximize the chances of early detection of congenital malaria, neonates born to mothers with malaria in the last 7 days before delivery should be investigated with a blood film for malaria parasites irrespective of the clinical picture and weekly thereafter for the first month
the clinical features of neonatal and congenital malaria overlap with sepsis syndromes. Other symptoms can include anaemia, jaundice, diarrhoea, vomiting, lethargy, convulsions, irritability, tachypnoea, respiratory distress, hepatosplenomegaly
for infants weighing less than 5kg with uncomplicated P. falciparum, the World Health Organization (WHO) recommends treatment with ACT at the same mg/ kg body weight dose as for children weighing 5 kg.
I’ll report back to the learners tomorrow. They do not look for malaria here in babies born to mothers with active malaria but the paper suggests that may be testing is indicated. We all learnt something today.
There’s more to language than the words that we say. Our learners are still wearing masks most of the time and gauging the mood of the lecture theatre is occasionally challenging. I was wondering why people were looking at me like I was crazy – it was the eyebrows. When Ugandans raise their eyebrows (at least in this part of Uganda) they mean “yes, definitely” (or “you can take it to the bank” as one of the Americans staying in the guest house with us put it). I saw it as an expression of doubt or enquiry so I was repeating the questions and getting more and more eye brow waggling. The manager of the guesthouse has a degree in applied linguistics but does not have a technical term for this.
Here I am, learning how to read people’s eyebrow talk
All 15 candidates passed the first course and we have identified 7 potential instructors who we will train later in the year (all being well with the fundraising). The standard was high overall and we were very impressed in particular with the learners’ level of engagement with the scenario / simulation training this afternoon. There is a sim lab in the nursing school here and it showed in the way everyone got involved. Well done everyone!
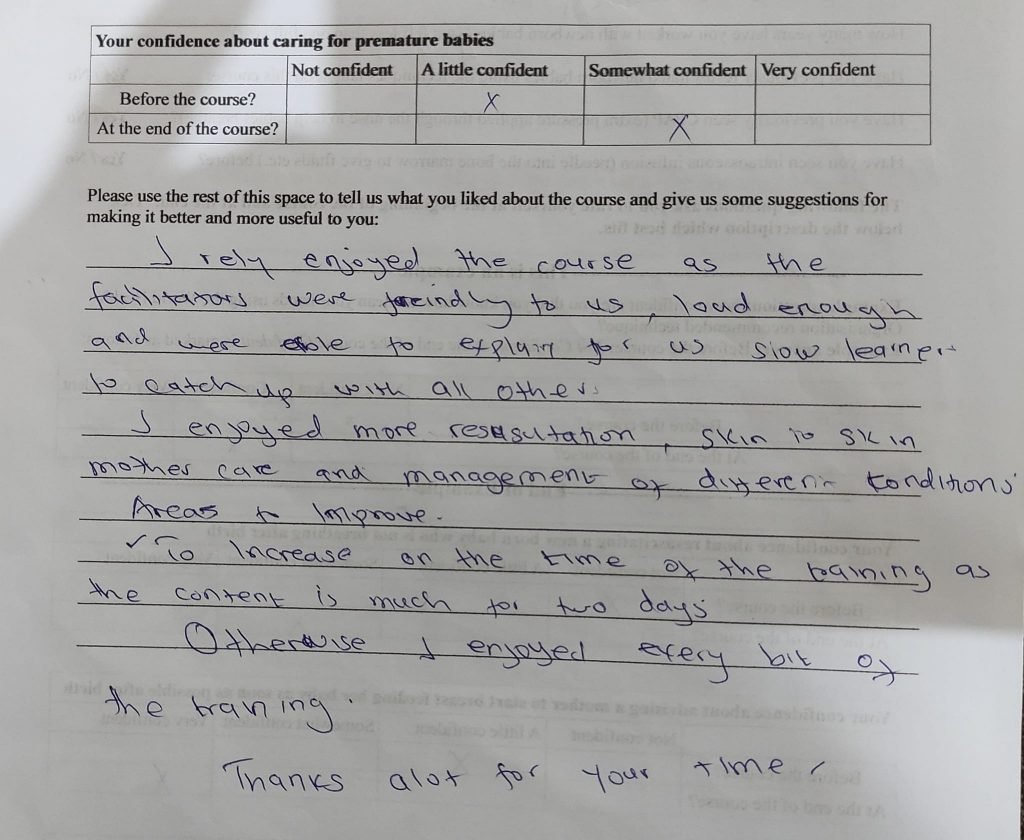
We are going through the feedback forms at the moment but here is a flavour. We collect information on confidence levels before and after a skill or topic is taught. An increase in confidence has been shown to correlate with an increase in competence because confidence empowers people to “give something a go”. If you lack confidence in resuscitating a baby, you might stand by and not even try when faced with a baby born with no respiratory effort. Whereas, if you think you might be able to achieve something, and at least position the baby’s airway so that when he/she gasps, air goes into the lungs, the likelihood of a positive outcome is infinitely increased.
A reassuring increase in confidence in 3 fundamental areas of neonatal care for this learnerWe received lots of positive free text feedback comments. And the common request to extend the length of the course.
Grace overseeing neonatal life support trainingKirstie lecturing on skin to skin mothercareTwins in skin to skin mother care on the neonatal unitJarlath running a breastfeeding workshop with our hastily knitted breast from yesterday as visual aid
Timings have been a bit of a challenge today: Devotions over ran, half our learners had to do a ward round before the teaching could start and Julia and Grace were called for clinical duties in the neonatal unit at lunch time as the paediatrician is away and a new 1kg baby was admitted. Jarlath and Kirstie did sterling work keeping the show on the road and we came in at 5.45pm with only one lecture left out and everyone still smiling.
NICHE International was set up to train local health professionals to teach the Neonatal Care Course (NCC). We follow the model used by life support organisations all over the world – clinicians do the course themselves, some are recommended as instructors, they train as instructors, form their own faculty with a bit of support initially from senior instructors, start training their peers and eventually begin to train their own instructors. The NCC sits under the umbrella of the Advanced Life Support Group (ALSG) in the UK.
The overall aim of the Neonatal Care Course is to reduce neonatal mortality rates (death of a baby in the first month of life).
The statistics above taken from https://www.healthynewbornnetwork.org/hnn-content/uploads/Uganda-CD2030.pdf, show that the neonatal mortality rate in Uganda reduced from 35 per 1000 live births in 2000 to 21 in 2016. 35% of the under-5s deaths though are in the neonatal period. The NCC can help bring down the numbers of deaths caused by complications of preterm births, sepsis and pneumonia. Together, these 3 causes make up half of the deaths in the first 28 days of life. We think that’s something worth working for.
Bwindi community hospital with the Impenetrable National Park as a backdrop
Bwindi Community Hospital cares for more than 120,000 people living in the South Western corner of Uganda. It was set up by American missionaries in 2003, starting as a clinic under a tree and expanding over the years to a thriving, award winning community hospital with 135 beds, a Nursing School with 400 students and Uganda College of Health Sciences Bwindi. Quite a bit of research goes on here, human and the other primates who inhabit the forest.
Grace, Kirstie and Jarlath admiring the banana plantation on the path between the hospital and nursing school
Tomorrow we start the course. We have 16 students for the Neonatal Care Course and are excited to get going. We’ve spent today setting up the room, finding spare tables, oxygen concentrator, remote control for the slides etc. Jarlath left his knitted breast in Ireland which we normally use for the breastfeeding workshop but the guesthouse manager’s daughter came up trumps and crocheted one for us last night with her last bits of yarn. So we’re all set.
12 seater plane Entebbe to Kihihi airstrip in south western UgandaJulia, Grace and Kirstie looking fairly relaxed en route to Kihihi
This was the 12 seater plane that brought us to Kihihi yesterday, the nearest airstrip to Bwindi Community Hospital. We were the only ones on it with our 2 pilots, and we are very grateful that we were allowed to bring the extra teaching equipment with us. The photos are reminiscent of Liberia in 2019.
Storm Eunice over the UK threatened our departure plans and Grace had fun and games with her visa from Cameroon but we all arrived safely and in good spirits.
It is just great to be out doing this again after 2 years grounded in our individual home countries. Flying over the the world’s largest and driest sand desert—the ‘Rub’al-Khali’— in Saudi Arabia, Yemen and Oman I felt like my world had opened up again. We are so very privileged to be able to volunteer like this, to be accepted into other people’s lives, to teach and to learn.