We’ve just finished Day 1 of the first Neonatal Care Course being taught by Ugandan instructors. All 12 instructors passed the Generic Instructor Course yesterday and rose to the challenge of teaching the NCC today. We are running this course in the chapel. Grace is course directing and made sure everyone knew the ground rules.
It wasn’t long before the newly trained instructors took over from us:
International Nurses Day is celebrated around the world every May 12, the anniversary of Florence Nightingale’s birth.
Felicia with baby manikins donated to or bought by NICHE, and used for training in new born resuscitation
The theme for 2022 is ‘Nurses: A Voice to Lead – Invest in Nursing and respect rights to secure global health‘
Working in neonatal care in Cameroon, Liberia and Uganda it is very obvious just how crucial good nurses are to the survival of all babies, but especially those who are premature or unwell.
We have also found ‘voices to lead’ among the nurses with whom we have worked, and seen their dedication and abilities.
Felicia is a nurse working in an isolated rural setting in Adamawa Region, one of the Regions in the North of Cameroon which has very high perinatal mortality.
Gathering the evidence for the work we do, both for funders and to inform our direction of travel as an organisation, is not at all easy! Alison has been working with Grace in Cameroon to collect information from health clinics about their use of bag-valve-masks which NICHE International provided them with a few months ago.
3 out of the 5 units who had the questionnaire responded which doesn’t give us statistically robust information but does give us a fascinating insight into the obstetric services at these centres, the numbers of deliveries, trained staff and how many babies were born in a bad enough condition to worry the newly trained personnel.
preliminary results from the BVM questionnaire
There are a couple of things to learn from here:
1.) The very positive free text comments at the bottom that all units feel that having the bag-valve-mask over the last 8 weeks has potentially saved lives.
2.) The disappointing comment from Bafoussam that people have been reluctant to use the BVM because they can’t attach it to the oxygen supply is a reminder of the need for on-going training and refresher courses. Babies born at 32 weeks gestation and above should be resuscitated in air. The new 2021 guidelines suggest that babies between 28 and 32 weeks can be resuscitated in air to 30% oxygen. Only the very small ones, most of which do not survive in resource poor areas of the world, should be resuscitated in 30% oxygen from the outset. It is recommended to increase to 100% oxygen in any situation if the baby requires cardiac compressions.
We are looking to return to Cameroon at the end of April 2022 to train more instructors and begin training some of the Cameroonian instructors to be instructor trainers themselves. Well done to Grace and team for keeping the Neonatal Care Course training going throughout the Covid pandemic and thanks to the Cameroon Baptist Convention for continuing to fund the programme.
Learning Curve: shows a relationship between the amount of practice / experience of a skill and the degree of competence achieved.
Forgetting Curve: the relation between the decay of a learned skill and the time elapsed since the skill was learned.
Experience Curves: combines the learning and forgetting curves.
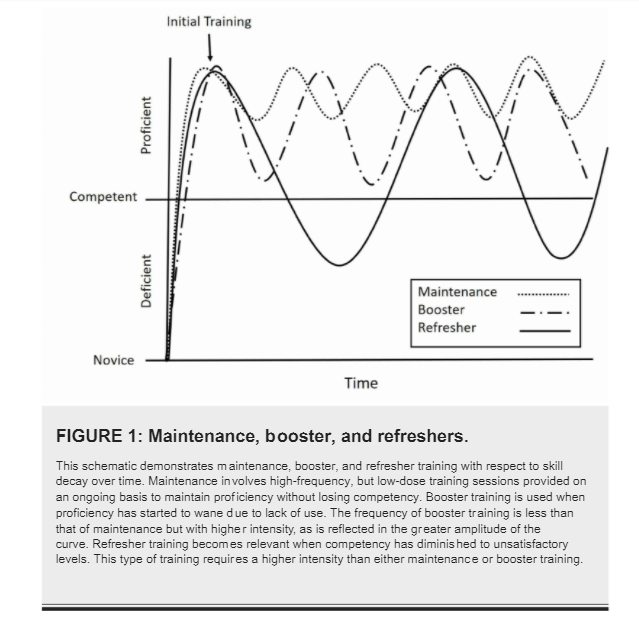
Activities to overcome skill decay can be qualitatively classified as maintenance , booster or refresher, according to the diagram below:
Note the amount of time spent “deficient” with “refresher” activities. An example of this is paediatricians in the UK re-certifying in APLS every 4 years. “Booster” training is possibly achieved by statutory mandatory training paediatric basic life support every year and keeps the average paediatrician “proficient”. Would lower intensity but more frequent “maintenance” activities do a better job eg. weekly simulation training sessions?
Here is Kola delivering his “booster” training sessions in neonatal resuscitation to nurse technicians in Liberia this week, using equipment left by NICHE after the first batch of instructors were trained in 2019.
Kola (centre) teaching neonatal resuscitation in Liberia, February 2021
How often does he need to run these sessions to make this maintenance training and not refresher sessions? The quest continues….
One of the slides from the NCC lecture on Nutrition and Feeding
This is a slide from one of the early lectures on the Newborn Care Course. It outlines WHO’s priorities in the fight to bring down neonatal mortality (number of deaths per 1,000 live births) to “at least as low as 12 per 1,000” by 2030.
Liberia’s neonatal mortality rate is 25 per 1,000 [UNICEF 2018 data]. 3 babies have died in the hospital in Zwedru since we’ve been here; 2 term babies born with severe hypoxic ischaemic encephalopathy (lack of oxygen around the time of birth) and 1 preterm baby weighing 900g who looked quite well when we arrived but died on day 6 of life during our second course – despite 2 of the local instructors leaving the course to go to the hospital to try and help save the baby.
Not many babies under 1.5kg survive here. Kola’s been discussing this this evening and showing us pictures of his successes – including one little lad called Success, born by perimortem Caesarean section to a mother with severe eclampsia, at 1kg. Now, developmentally normal and with adoptive parents, the family recently came back to the unit to celebrate his second birthday. Kola’s smallest survivor weighed just 600g at birth at 29 weeks gestation. He is now over 1 and also developmentally normal. I suspect that although the survival rates at different gestational ages are very much lower than in the UK, the percentage surviving without severe disability is probably higher.
Kola’s turns of phrase when he’s lecturing have been delighting Jo and I all day. The title of this and the previous posts are good examples of the fervour with which he plays his role as MCAI’s on the ground neonatal trainer. And he is not alone. Gertrude, Agnes and Christina are equally dedicated to their patients and their unit, totally committed to the patients they look after. And totally engaged in their roles today as instructor candidates on the Newborn Care Course.
Gertrude doing Stage 2 of the 4-stage procedure in how to tie a kalafong wrap for the baby to be skin-to-skin with its mother.
Christina overseeing resuscitation skills training.
Agnes (gesticulating with her hands) running an animated discussion workshop on pain in babies and how to manage the baby who won’t live long.
The ultimate outcome measurement for the Newborn Care Course project would of course be a reduction in neonatal mortality in the areas where we work. There are so many confounding factors in any clean data that is actually collected that it is almost impossible to prove that one intervention like this has any statistically significant effect on neonatal mortality. But our funders always ask for outcome measures. This year in Cameroon we changed the feedback form a bit, bringing it more into line with the template suggested by the UK’s Royal College of Paediatrics and Child Health. This has allowed us to measure pre- and post- course confidence in the main areas identified by WHO as contributing to newborn deaths. Here are the results from last month’s course:
The challenge now, of course, is to keep that confidence up going forwards.
It was noticeable that when Cameroonian candidates were role-playing a scenario, for example giving the baby to the mother after a successful resuscitation, they would speak to her in Pidgin English (sometimes called Kamtok in Cameroon).
One of the candidates used the sentence above. It means ‘the baby hasn’t died’.
It is a reminder that neonatal mortality in Cameroon is still 10 times that in the UK, and that the aim of teaching the Newborn Care Course is to reduce it.
48 of the 49 candidates who took part successfully completed the course in April 2019. That’s 48 more skilled birth attendants and nearly 20 trained or partially trained instructors (not all those who did the GIC last year managed to get to these courses to do their supervised teaching) who will continue to cascade the learning. That’s good news for many thousands of babies in Cameroon in the years to come.
With some French and some English speakers (and some hard to understand UK accents) we wanted to be sure that learners could hear and understand everything they were being taught. Jarlath initiated his ‘traffic light system’, whereby everyone was given a piece of paper with a red light drawn on it. They were asked to hold up the red light if they couldn’t hear or understand what was being said. It works well with learners who are too polite to say they don’t follow.
We are very lucky to have such senior instructors involved with NICHE. Their breadth of experience is humbling for those of us still hanging on their coat tails, they can adapt their teaching style to any situation, they are supremely patient with the learners and they never, ever, pass up an opportunity to pass on skills and knowledge – even if the only flat space available is a windowsill a few floors up (thank goodness it’s only a manikin).
On the NCCs at the end of April in Cameroon, altogether we had candidates from 6 of Cameroon’s 10 Regions. Participants came from a variety of work places, some small local health centres, some bigger hospitals. There were nurses, midwives, doctors and a paediatric surgeon taking part. There were English and French speakers. The workshops and small group teaching gave participants the chance to share their experiences, and discuss specific problems that they face at work. This is important in a health environment where doctors and midwives and nurses do not usually share training experiences.
Paediatric surgeon, George, practises resuscitating a baby
Midwife, Julia, studies her course manual. Julia did particularly well on the course and is responsible for training other midwives in her health facility in Douala. NICHE left one of the manikins donated by the BMA with her so that she can continue to cascade what she learnt to others.